Submissions from Readers
Nasogastric Tube Feeding and Assessing Readiness for Oral Feeding
Question: If the patient has a nasogastric tube, how do we assess that the patient is ready for oral feeding?
Answer: The patient can be evaluated by a speech therapist and have a videofluoroscopic swallow study (also known as modified barium swallow study) performed. This study is done via x-ray while the patient is given different foods and drink to swallow that are mixed with barium. The barium allows the food and drink to show up on the x-ray and is not harmful. The speech therapist and M.D. can then determine if the patient is ready for oral feeding and if a modified diet is needed (i.e. thickened liquids, pureed food, etc.) The nasogastric tube will not interfere with the study.
Comments for Nasogastric Tube Feeding and Assessing Readiness for Oral Feeding
|
||
|
||
Self Feeding After Stroke
by Amy
(Nashville, Tn, USA)
Question:If you have a client who has a Goal of feeding himself with set up and supervision by d/c and he has had a R CVA, L flaccid hemiplegia with poor sitting balance, what would be some things to do with him to help him meet his goal?
Answer: You need to work on the following:
Balance
Positioning
Use of non-dominant hand (if applicable)
Coordination
Ordering any adaptive equipment
Vision
Education about pocketing food
Swallowing issues (with aid of speech therapist)
Work to improve sitting balance. I find that most patients can learn to sit up independently prior to d/c even with flaccid hemiplegia. Any activity will be difficult if the patient cannot sit up so that is always one of the first things I work on. If the patient has had an extremely severe stroke and cannot sit up after extensive rehab, then you will need to make sure they are positioned safely in their w/c to perform feeding.
If the patient is flaccid on their dominant side, they will need to learn to feed themselves with the non-dominant hand so actually practicing with the non-dominant hand is important since it will be awkward. Coordination exercises may be necessary if coordination has been affected.
You may need a plate guard to keep food from spilling from their plate or even curved utensils if coordination is an issue.
Another aspect of feeding involves making sure you educate the patient about pocketing of food on the weak side and how to clear the food with the tongue. If the patient has swallowing issues, the speech therapist can educate the patient on the appropriate techniques to improve swallow function.
You will also need to make sure the patient doesn't have any visual field deficits or hemianopsia. If a patient does have these issues, then it is important to have them learn to scan further for food or to have the caregiver set the plate further toward the strong side in the patient's line of vision.
Have the patient practice, practice, practice!
Comments for Self Feeding After Stroke
|
||
|
||
|
||
|
||
Drooling After Stroke
by Johan
(Kuala Lumpur Malaysia)
Question: How can I reduce excessive drooling and cut down on thick mucous build-up?
Answer: Drooling and excessive salivation which is called sialorrhea can be a problem following stroke. It is often caused by poor control of oral and facial muscles. It can also be caused by decreased sensation, poor posture, or other factors such as dental malocclusion or increased production of saliva. Some of the treatment options for sialorrhea include:
1) Speech therapy including oral and facial exercises to strengthen musculature - you can find sample oral motor exercises at www.speech-therapy-on-video.com/oralmotor.html
2) Positioning devices to improve posture
3) Orthodontic plates that can aid in better lip closure
4) Medications that block the parasympathetic innervation of the salivary glands
5) Injection of botulinum toxin into the salivary glands (must be repeated because effects wear off after several months)
6) Surgery to denervate the salivary glands
Here is an article that gives more depth information about management of sialorrhea:
www.aafp.org/afp/2004/0601/p2628.html
I would first try speech therapy or exercises to strengthen your oral motor control. If that doesn't work then I would talk to a physician or dentist about other options.
Dysphagia and Swallowing Difficulty
Question: Are there any techniques to stop coughing when drinking? I know about using thickeners but wonder if there were drinking techniques?
Answer: There are compensatory swallow techniques that speech language pathologists (SLPs) use with some stroke patients to improve swallowing. It is impossible to tell if the strategies are successful unless they are observed during a video fluoroscopy with a modified barium swallow so it is not advisable for an indivual to try strategies on their own. One should consult a SLP to determine which strategies to use. A SLP can instruct patients on what strategies may work and can verify that the strategies are successful through video fluoroscopy.
Some common swallow strategies that are used are upright posture when drinking, small sips, no straws, chin tuck when swallowing, and alternating food with drink. There are also exercises the SLP can do with a patient to strengthen the muscles involved in swallowing.
Aspiration occurs when liquid or food travel down the windpipe into the lungs rather than the esophagus. Aspiration can be silent without any symptoms, cause pneumonia, and can be fatal so it is very important to follow whatever precautions the SLP advises.
by Deedy
(Georgia)
Question: My 25 year old son dove into a pool on August 2009, 1 year and 5 months ago. He fractured C5 and C6, C7 was shattered and compressed the spinal cord. He had 2 neck surgeries by a neurosurgeon. They kept him asleep with medications for several days, he had a tube down his throat at the time, on a vent. When he woke up we noticed he was not using his left side very well, his eye would not turn to the side and his face was a little drooped on that side, arm and leg was weak. He is an incomplete quad, but now has use of his arms, but not his fingers and no movement from about under the rib cage down. He still has feeling, he can tell you where and which toe you are touching. Not much sense of hot and cold. He lost his swallow and had to have a trach put in and peg feeding tube, because of weak swallow. He has had some swallow therapy. They did the e-stim treatment once, but said the swallow muscles are working now, the epiglottis just sticks up straight and will not flap down over teh windpipe to keep anything by mouth from going into his lungs!! We have to suction him from the trach. He is no longer on the ventilator, but does require it at night sometimes, because he has had several bouts with pneumonia. My question, I hope you can please help us with, is there any chance that the epiglottis will start working again on it's own? How long could this take, if at all possible? Is there any clinical trials here in Georgia or USA? Is there anything or anywhere we can get treatment or surgery to correct the epiglottis? Please help, we are desperate. Zack is 27 now and may never walk again. He has a power wheelchair he can drive. Right now the swallow is our concern, so he can eat and drink, and get the peg tube and trach out to much improve his quality of life. Please, please send any info that may help my son, Zack! God Bless You , DEEDY (ZACKS MOM)
Answer: This is really a question for a physician who deals with swallowing dysfunction as well as a speech language pathologist. I can give you some ideas of where to get information or where to search.
Go to Clinicaltrials.gov and enter your keyword to search for clinical trials. Some keywords you should try (separately) are deglutition, epiglottis, and dysphagia. You can see all the current studies that are seeking participants. Once you perform your search, there will be a link toward the upper left corner to click that says "hide studies that are not seeking new volunteers", which will narrow your search.
Go to Speechpathology.com to their askexpert page. You can scroll through answers to dysphagia questions, and you can also submit your own question.
Some other search terms to do via a search engine (Google, Yahoo, etc.) would be:
Treatment of deglutition disorders
Dysphagia Clinical Trials
Deglutition Clinical Trials
Surgical treatment for dysphagia
Surgical treatment for deglutition
Treatment for epiglottis dysfunction
Hopefully, you can find a better answer to your question at one of these resources. Good luck and God Bless You!
Where does food pocketing occur if you have left CVA?
by Annabell Baret
(Canada)
Question: If a client had a left CVA, where may pocketing of food occur?
Answer: Typically, a stroke that occurs in the left side of the brain will affect the right side of the face thus pocketing would occur on the right. There are some exceptions to this though depending on what structure of the brain is affected.
Refusing to Eat
by Eileen
(Massachusetts)
Question: My mother had acute stroke 2 months ago. She has thrush in her mouth and is refusing to eat. She has experienced small type stroke on her other side but nothing too serious and they want her to return to rehab. Rehab does not want her until she eats. She has very good return on her right side and is just on the verge of walking and can pick up her right arm. What do we do - should we put in a feeding tube?
Answer: This is definitely a medical question rather than a physical rehabilitation question so I would tell you to consult the physician. Obviously you want to make sure she is getting treated for the thrush. If she is not getting enough nutrition, and the MD feels a feeding tube is appropriate, then I would follow their advice. An inpatient rehab will accept someone with a feeding tube, and the doctors can write orders allowing her to physically eat and only supplement with the feeding tube as necessary until she can tolerate fully eating by mouth.
Hemorrhagic Stroke and Aspiration Pneumonia
by Emilly Reno
(Birmingham)
Question: My Dad had a hemorrhagic stroke five days ago. The neurologist said he would never be able to move his left side but within one day he was raising his left leg - still can't move his left arm but the medical team work with him everyday. His speech is better but I don't understand why he can't have one drop of water, his mouth is full of dead skin and he is so begging for water. The neurologist said if one drop of water reaches his lungs that he could get pneumonia. I don't understand, please explain.
Answer: A stroke victim's swallowing can be affected, and some patients cannot drink any liquid because it goes into their lungs rather than their stomach. This process is called aspiration. Aspiration pneumonia can occur as a result which can be deadly. Varied sources report that 15-31% of stroke related deaths are due to aspiration pneumonia so it is very serious. Please do not give any liquid to your father without being instructed to do so.
The hospital should have special swabs that can be used to moisten his mouth/lips. You could also request that the MD write some type of order for staff to address your dad's oral care at least twice a day if you feel that it is not being done. One of the risk factors for aspiration pneumonia is bacteria in the mouth and poor oral care so it is important that they are cleaning the oral cavity. The swabs mentioned above do not clean the mouth. They only provide moisture relief. The moisture relief will help with the dryness, but make sure that oral care is taking place as well. If you want to learn more about it, you can do an online search of oral care and dysphagia or oral care and aspiration pneumonia.
Not eating
by Chris
(MI)
Question: My mother had a left brain stroke with aphasia 2 1/2 months ago. She has her mobility and still attends speech and language therapy, however, she barely eats. She says she is not hungry and has lost 35 lbs. in 2 1/2 months and is extremely tired all the time. Recently, she went back in the hospital for a day for dehydration. She says there is no issue with swallowing (was tested for this) or metal taste in the mouth. How do I get her to eat? What do I do to help her get some calories, nutrients in her body and gain weight? Everything I have tried she will take a bite of.
Answer: There are shakes such as Ensure and Boost to help those who need more nutrition. There are also protein packets or liquids that can be added to drinks. I would seek the help of a nutritionist who can give you some ideas of some higher calorie foods or supplements that can be used. Plus, a nutritionist could help you know what foods to avoid that would not be good for her due to health conditions (thought this may not be as important since she is barely eating). I would focus on higher calorie foods like avocados or peanut butter rather than a larger quantity of food. You could also talk to her MD to see if an appetite stimulant might be appropriate or to find out if any of her meds are affecting her appetite.
Eating Difficulties
by Martyn Wainwright
(Dorset UK)
Question: What food should the stroke victim never eat?
Answer: Some people who have had stroke have other diseases or complications that would prevent them from eating certain types of foods. For example, a diabetic wouldn't want to eat sugary foods or someone with dysphagia or swallowing problems may not be able to eat certain foods or drinks (or may not be able to eat at all) due to aspiration risks. If someone does not have any precautions/diseases that prevent them from eating certain types of food, then the best recommendation is to eat healthy foods that decrease the risk for stroke or cardiovascular disease. Nutrition guidelines have been set up by the American Heart Association and can be viewed at: http://stroke.ahajournals.org/content/31/11/2751.full. It may be okay to splurge on an unhealthy food on occasion, but it is best to follow healthy nutritional guidelines to help decrease risk of another stroke.
Drooling
by Mary Ann
Question: Hi, I hope you have some ideas for me. My stroke was an ischemic stroke in 2017. In the past 3 years, I have had intermittent drooling from both sides of my mouth with no control. It just comes. I have tried Botox and Acupuncture to no avail. My neurologist wants me to take medicine which I don’t want to do. Thanks
Answer: I would suggest seeking guidance from a speech-language pathologist (often called a speech therapist). They can conduct a thorough swallow test to identify any difficulties and offer various strategies to address the problem. Some areas the speech therapist may be able to help you with include:
Oral Exercises: Engaging in specific exercises that target the muscles involved in swallowing can help improve control and coordination.
Posture Adjustment: Altering your posture while eating or drinking can assist in reducing drooling.
Behavior Modification: Implementing conscious behavioral changes, such as practicing lip closure or swallowing techniques, can help reduce drooling.
Some other suggestions for managing drooling include:
Non-invasive Stimulation Techniques: Certain non-invasive techniques, such as transcranial magnetic stimulation or electrical stimulation, may be utilized to modulate the neural pathways involved in swallowing and saliva control. These techniques should be administered under the guidance of a healthcare professional.
Kinesiotaping: Here is a website that shows a kinesiotaping technique for managing drooling: https://www.thysol.com.au/kinesiology-tape-applications/excessive-drooling/". There are various taping techniques, so you could search for a kinesiotaping professional near you that could help.
Oral Devices: Certain oral appliances or devices can be utilized to enhance oral control and prevent excessive drooling. These may include specially designed mouthguards or oral splints that promote better swallowing.
You can consult with a healthcare professional or speech-language pathologist to determine the most appropriate strategies for your specific situation. They can provide personalized guidance and help you find the best combination of approaches to manage drooling.
Treatment Tips from Others
To see tips from other survivors and caregivers about their treatment recommendations, click here.
Get Our Stroke Rehab Guide


Our stroke rehab guide is designed specifically for patients and caregivers. It's in pdf format and can be immediately downloaded. It includes about
- Stroke Definition & Causes
- Stroke Treatment
- Rehabilitation Information for Physical, Occupational and Speech Therapy
- Exercise pictures
- Q&A from patients and caregivers
- Adaptive Equipment & Techniques
- How to Prevent Another Stroke & More!
Medical Disclaimer: All information on this website is for informational purposes only. This website does not provide medical advice or treatment. Always seek the advice of your physician or other healthcare provider before undertaking a new healthcare or exercise regimen. Never disregard professional medical advice or delay seeking medical treatment because of something you have read on this website. See the disclaimer page for full information.
- Home
- Stroke Questions
- Drooling
Recent Articles
-
Stroke Recovery Tips Back Issues from Stroke Rehab Website
 View past issues of Stroke Recovery Tips Newsletter to learn unique information about stroke rehabilitation.
View past issues of Stroke Recovery Tips Newsletter to learn unique information about stroke rehabilitation. -
Gift Ideas for Stroke Patients for Recovery, Comfort & More
 Top gift ideas for stroke patients and stroke recovery and rehabilitation.
Top gift ideas for stroke patients and stroke recovery and rehabilitation. -
Jerking Movement After Stroke
Question: Why is there a sudden jerk on the paralyzed/flaccid side of a stroke patient? Is it normal or not? Answer: Here are a few of the reasons stroke -
Hand Exercises for Stroke by Certified Hand Therapist
 Hand exercises for the stroke patient that will improve fine motor skills.
Hand exercises for the stroke patient that will improve fine motor skills. -
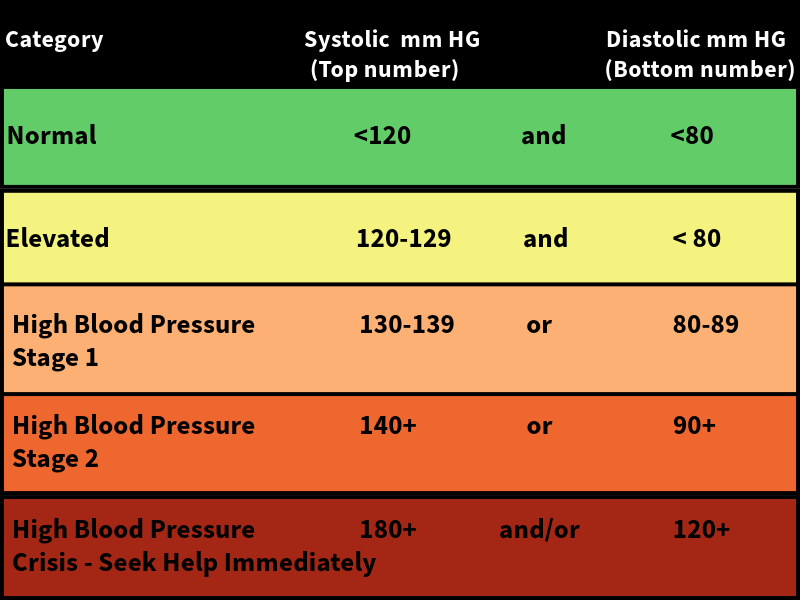
Stroke and High Blood Pressure
 The silent killer - understand how stroke and high blood pressure are related.
The silent killer - understand how stroke and high blood pressure are related. -
Are Strokes Hereditary? Understanding Your Risk Factors
 The Question: Are Strokes Hereditary? The Answer: Genetics can play a significant role in determining one's risk.
The Question: Are Strokes Hereditary? The Answer: Genetics can play a significant role in determining one's risk. -
What is apraxia caused by a stroke and how to treat it
 What is apraxia and it's various forms that occur after stroke including speech, ideational, and ideomotor apraxia.
What is apraxia and it's various forms that occur after stroke including speech, ideational, and ideomotor apraxia. -
Caregiver Questions and Issues
Questions and answers from Stroke Caregivers